Hypertrophic cardiomyopathy, also called "H.C.M.", is the most common inherited cardiac condition, affecting up to 500,000 Americans. Worldwide, approximately 1 in 500 individuals are affected. HCM is caused by abnormally thick muscle in the heart. Symptoms of the disease depend on where this abnormal muscle is located within the heart’s structure, and can range from severe, life-limiting symptoms to nothing at all.
Advertisement
What causes HCM?
The muscle of the heart is very special. Unlike other types of muscle in the body, cardiac muscle is made to work constantly throughout our lives. Many genes are involved in the making of cardiac muscles. Mutations in the genes that form the cardiac muscle cause the formation of abnormal muscle. The mutations responsible for the development of hypertrophic cardiomyopathy are autosomal dominant. This means that most people who have the condition have one parent who shares it, and it’s very likely they will pass it to future generations.

Looking at the heart muscle of a patient with HCM under a microscope will show muscle cells that are very different from those in the heart of a healthy individual. The organized structure of normal muscle is lost, and the cells are bizarre looking and in disarray. The type of muscle formed by these mutated genes is abnormal in different ways. Abnormal muscle is thicker than normal heart muscle. Also, regular functions of normal heart muscle, like squeezing and relaxing, can be impaired. Abnormal heart muscle can also be "arrhythmogenic", meaning that it can spontaneously trigger a dangerous arrhythmia in the heart.
Hypertrophic Cardiomyopathy and the Risk of Sudden Cardiac Death
HCM is often thought of as one of the most important causes of sudden cardiac death (SCD). Studies in large populations suggest HCM may be the cause of SCD in anywhere between 10 percent and 30 percent of all cases. How HCM causes sudden cardiac death is complicated, and probably varies from case to case. Cardiologists who manage patients with HCM evaluate this risk in great detail, looking at different factors including family history, severity of the condition and symptoms present. If a person suffering from hypertrophic cardiomyopathy is thought to be at high risk for sudden cardiac death, an implantable defibrillator may be recommended.
The question of whether all athletes should be screened for the condition remains a gray matter.
Athletes who are already diagnosed with the condition are currently advised to avoid strenuous exercise, although the amount of exercise that exposes an HCM patient to a higher risk of sudden cardiac death remains unanswered.
Obstructive HCM vs. Non-Obstructive HCM
Abnormally thick heart muscle fibers can appear in different parts of the heart. The location of the abnormal muscle within the structure of the heart affects how HCM feels to the person who has it. If the abnormally thick muscle fibers are located in the part of the heart where blood exits towards the body, they can block its path by making this passage narrow. This condition is called ‘hypertrophic obstructive cardiomyopathy’ or ‘HOCM.’

These fibers can also appear in the apex of the heart. The "apex" of the heart is the term doctors use to describe the end cone of the left ventricle. Apical hypertrophic cardiomyopathy was first described in Japan, and is commonly referred to as Japanese variant. There are also other ways HCM can present. Thickened muscle can appear in different walls of the heart. Even when not obstructing blood flow, HCM has the potential to cause trouble. An excessively thick heart loses many of its normal abilities to squeeze blood out (systole) and relax back to fill itself with blood (diastole). Some HCM patients can struggle with heart failure because the abnormal heart cannot meet the demands of the body.
How is HCM Diagnosed?
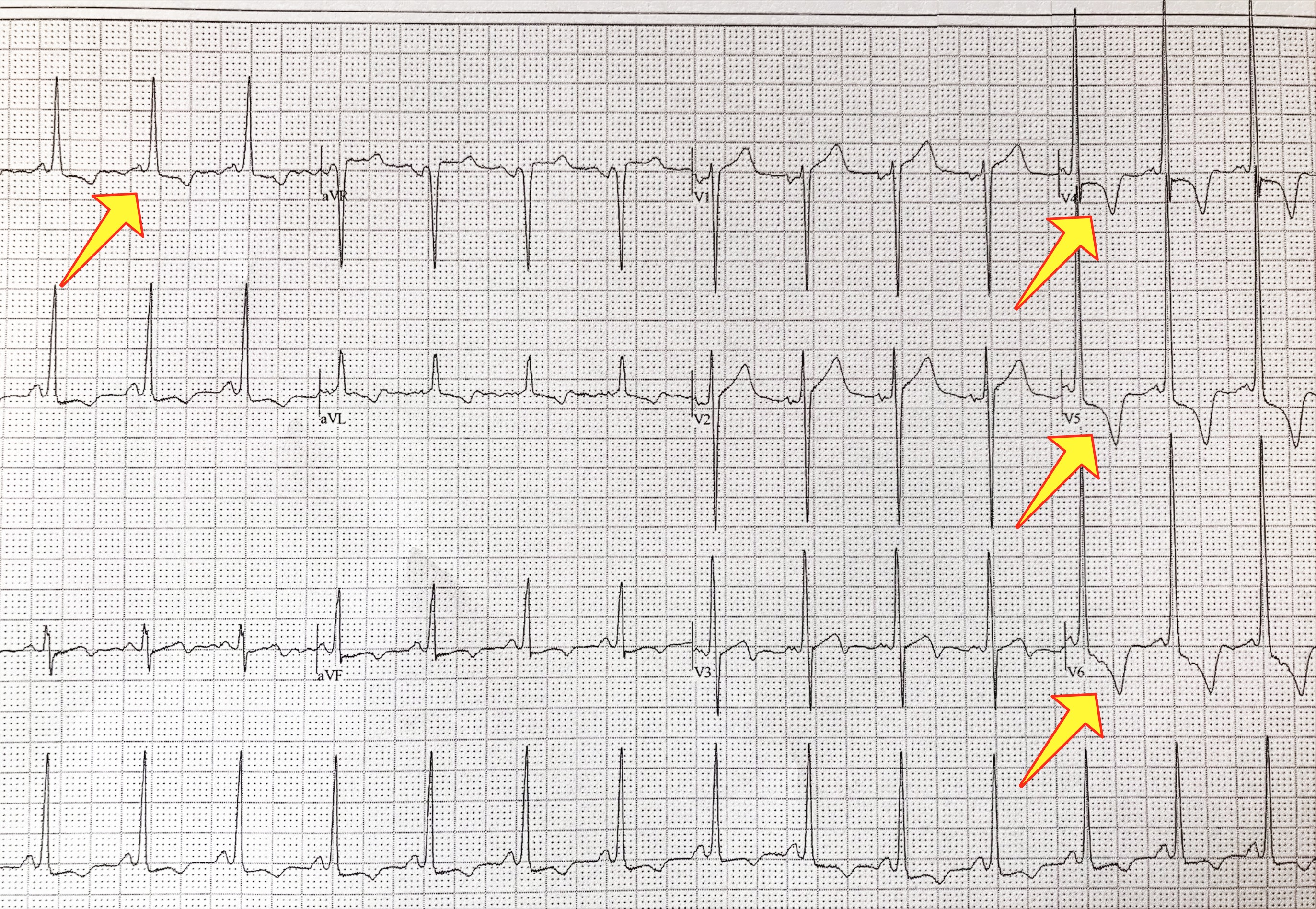
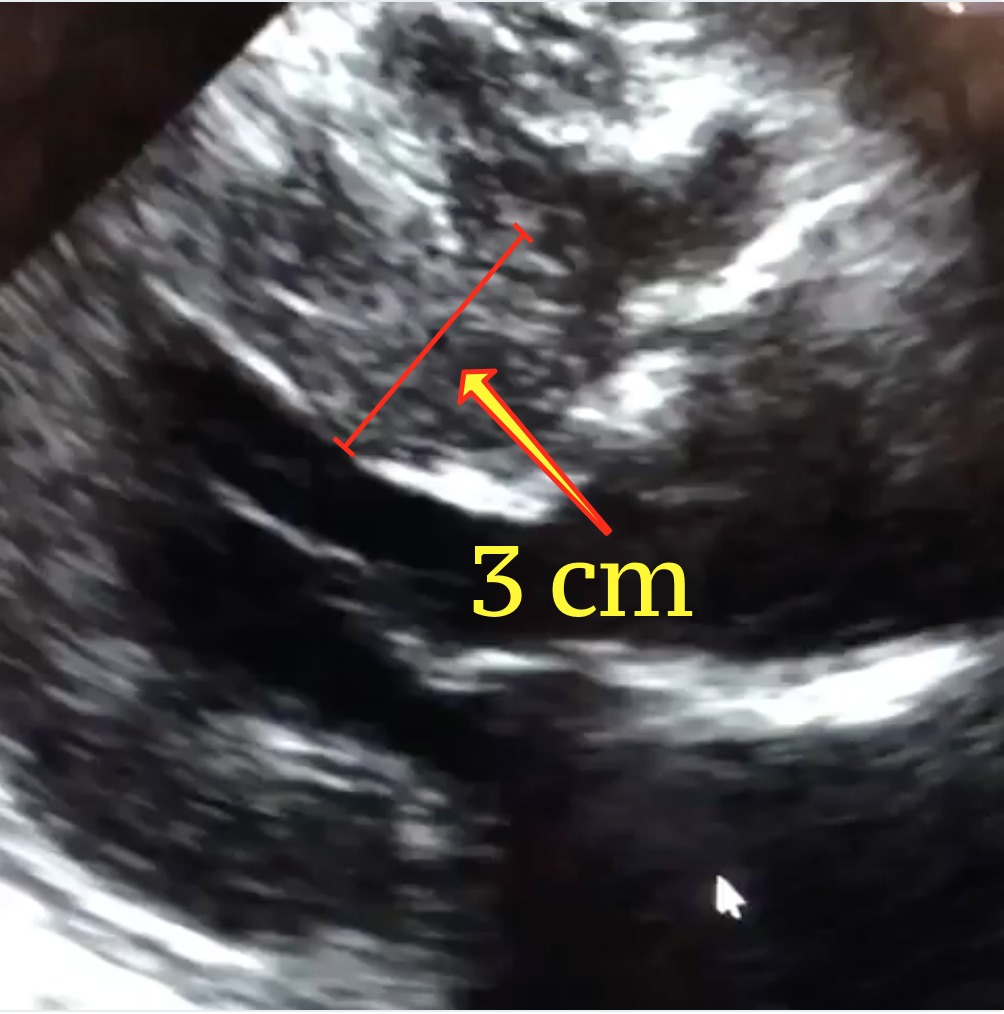
The echocardiogram is the test of choice to diagnose hypertrophic cardiomyopathy. Echo can identify the thickened muscle, measure it, and quantify the effect the abnormal muscle may be having on normal blood flow. The electrocardiogram of a patient with HCM is most often abnormal, and can help shed light on the condition; it is an excellent screening tool for HCM. This is one of the reasons why cardiologists obtain a baseline ECG on patients they see for the first time. In recent years, the cardiac MRI has emerged as one of the most important imaging tools for the heart because of its ability to create highly detailed pictures. A cardiac MRI can help diagnose HCM with great accuracy. It can detect even small amounts of thickened muscle that can be missed on echocardiography.
The technology to diagnose HCM with a blood test is in development and has not been fully developed in clinical practice. This is because only about 35 percent of HCM cases can be linked to a known gene that can be tested for. Also, it is still not clear how many cases of HCM appear from scratch, without a parent to inherit them from. Today, most of the screening for the disease is done by evaluating close relatives of the person affected. The echocardiogram and ECG are most often used for screening. Especially in younger people, screening may involve repetitive testing throughout life. If a causing gene is identified in a person suffering from HCM, then the same test can be used to diagnose other members of the family that could be affected.
What Does HCM Feel Like?
Cardiologists define the symptoms caused by HCM as "dynamic" because the can change from day to day depending on a variety of different conditions.
Symptoms of HCM can vary from person to person, and range from severe to nothing at all. The heart is constantly at work, and its normal function of pumping blood is affected by a variety of different factors, including your blood pressure and how well hydrated you are. Therefore, the effect of HCM on the way you feel can vary from day to day. Cardiologists describe the type of obstruction HCM causes on the heart as dynamic. People with HCM describe having good days, when they feel fine, and bad days, when minimal exertion causes symptoms. Common symptoms include shortness of breath with activity, and chest pain.

How is Hypertrophic Cardiomyopathy Treated?
Treatment for hypertrophic cardiomyopathy is intended to reduce the symptoms the condition causes. Shortness of breath is most often caused by the obstruction of blood flow into the body by the thickened muscle fibers. Medical therapy includes medications like beta blockers and calcium channel blockers that reduce the squeezing of the heart, and in turn reduce the amount of obstruction these muscle fibers cause. Doctors treating HCM are also careful to remove medications like diuretics and vasodilators that may make such obstructions worse.
For those who continue to experience symptoms even after medications have been adjusted, there are procedures both surgical and non-surgical designed to get rid of the obstruction. The surgery used for this purpose is called a septal myectomy (meaning removal of the muscle of the septum), and it involves cutting a piece of the obstructing muscle. For patients too sick, old or frail to undergo open-heart surgery, there is a procedure available known as a septal ablation that can also help. Septal ablations are performed via catheter, and can relieve the obstruction of blood flow caused by the abnormal muscle.
About the Author
Share this with a patient or friend
Advertisement